Septal Myectomy and Septal Ablation for Hypertrophic Cardiomyopathy
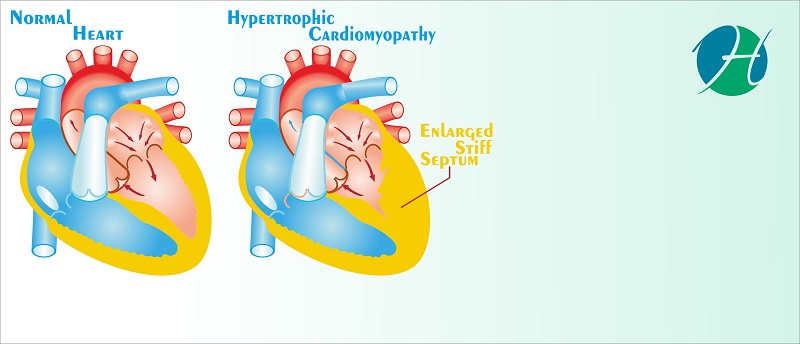
Hypertrophic Cardiomyopathy (HCM) is a genetically mediated, structural defect in the heart which results in an abnormally thickened muscular septum between the right and left ventricles. This thickened septum impedes blood flow out of the ventricles, particularly between the left ventricle and aorta (which supplies blood to the rest of the body). This most commonly presents as fainting spells in young adults, during exertion and can also result in sudden cardiac death.
Management of HCM is usually initiated with medications. If medicines fail to control the condition or in case of severe abnormalities in the structure and function of the heart, procedures such as septal myectomy and septal ablation are considered. Both procedures involve the removal of a part of the thickened septum to establish adequate blood flow, however, they differ in their approaches and have their own set of advantages and disadvantages which need to be considered before making a choice.
Investigations and Tests
The following tests are performed in all individuals with HCM considered for a procedure
- Echocardiogram: This test utilizes ultrasound waves to examine the structure of the heart. The blood flow between different heart chambers and into the blood vessels can also be measured. This is important in providing information on the blood flow between the left ventricle and the aorta in patients with HCM.
- Chest X-ray
- Electrocardiogram: This measures the electrical activity in the heart. It is recorded using skin electrodes placed on the chest
- Routine Blood investigations
- Cardiac Catheterisation: This test involves inserting a catheter (thin tube) into the heart chambers. The catheter is inserted through one of the blood vessels in the arm and pushed up to the heart. A dye inserted through this tube can be visualized using X-ray and allows for visualization of the cardiac blood supply. With an additional probe at the tip of the catheter, pressure differences between different parts of the heart can also be measured.

Septal Myectomy
Septal myectomy is a surgical procedure with open-heart surgery, where the chest is opened up to reveal the heart. The septum is accessed by passing through various heart structures. A portion of the thickened septum is cut surgically to establish normal blood flow from the left ventricle to the aorta, after which the chest is closed again.

Preparation
Prior to the surgery, a complete evaluation of the individual is done. As this procedure requires general anesthesia, an anesthetist is involved in care. Routine medications including those for other chronic illnesses are evaluated and may be modified prior to surgery. The individual will be instructed to avoid eating after midnight.
During the procedure
On the day of surgery, the individual would be placed under general anesthesia after which the surgeon would begin the procedure.
The chest is opened up by cutting through the sternum (breast bone) in the center. The individual is placed on a heart-lung machine. This machine carried out the work that is normally done by the heart and lungs (pumping blood and breathing). This allows the surgeons to handle a ‘still heart’.
The heart is visualized and the septum is accessed through passing through the heart muscles. The extra portion of the septum is removed from the left ventricle outflow tract, providing adequate blood flow to the aorta.
Often, surgeons would also plan to correct any defects in the mitral valve (the valve between left atrium and ventricle) as this is commonly distorted in individuals with HCM, causing a leak across the valve.
After the procedure is complete, temporary pacing wires may be left in place. This is done to provide electrical support to the heart. A chest drain is left to drain out excess fluid after which the chest is closed and sutured. The individual is then brought out of anesthesia and taken to a recovery room.
The entire procedure can take between 3 to 6 hours.
After the procedure
Regular monitoring of vitals with a focus on cardiac monitoring is carried out by specialists in an intensive care setting. There may be a pain in the chest, especially over the sternum where the chest was opened.
Occasionally, there may be a requirement for cardiac pacing and some individuals may have abnormal cardiac rhythms, requiring an ICD (implantable cardioverter-defibrillator), which records and corrects these abnormal rhythms.
Special instructions for follow up and wound care are provided, along with detailed instructions regarding medications. After 5 to 7 days, the individual is ready to be discharged.
SEPTAL ABLATION
This is a non-surgical procedure, where the chest is not opened. The abnormal septum is accessed using a catheter, a thin tube inserted through a blood vessel in the groin. The procedure is also called alcohol septal ablation, as alcohol at higher percentages is toxic to the heart muscle tissue and when used in the region of the septum, kills the extra tissue leaving thinner scar tissue.
Septal ablation is a newer procedure and is preferred for the elderly and those with other medical conditions that are contraindications to surgery.
This procedure is done without general anesthesia in the Cardiac Cath lab by your cardiologist and their team.

PREPARATION
A complete evaluation is done with the appropriate tests listed above. Routine medications are reviewed and some may be modified or stopped. The individual will be asked to refrain from eating after midnight.
DURING THE PROCEDURE
On the day of the procedure, the individual may be given medication to help relax. He or she would be conscious during the procedure. Aspirin and Heparin are given before beginning the procedure as blood thinners to prevent blood clots.
The groin is cleaned and anesthetized. The catheter is inserted into the vessel by piercing through the skin. The catheter tip is pushed and guided up until it reaches the heart. The position of the catheter tip is confirmed using echocardiography or by inserting a dye which can be detected by X-rays.
Once the tip is close to the abnormal septum, pure alcohol is inserted through the catheter. This destroys the excess septal tissue. There may be some discomfort experienced during this process. After this, the catheter is withdrawn from the heart and through the opening in the groin, following which the area is closed with sutures.
The entire procedure takes only 1 to 2 hours.
AFTER THE PROCEDURE
The individual will be monitored in the cardiac ICU for about a day to look for any abnormal rhythms. Vitals and routine parameters are checked periodically. An echocardiogram is performed to visualize the septum to see if the procedure has been successful in removing the extra septum. The area should appear as scar tissue.
It is important to lie down flat for a few hours after the procedure and avoid bending the hip. This is necessary to prevent excess bleeding from the incision in the groin.
After 1 to 3 days of observation, the individual is ready for discharge.
COMPLICATIONS AND RISKS OF SEPTAL MYECTOMY AND SEPTAL ABLATION
- Bleeding from the incision site
- Bleeding internally from damage to major blood vessels
- Infection and sepsis
- Arrhythmias or abnormal heart rhythms
- Blood clots
- Damage to heart tissue, including valve damage
- Damage to coronary vessels and risk of MI
Myectomy, being an open heart surgery takes longer to recover from and is not tolerated well by elderly individuals and those with other severe medical comorbidities. Septal ablation may pose fewer health risks, but has a higher chance of procedure failure and a higher risk of abnormal heart rhythms and a requirement for the pacemaker.
The final decision on the procedure should be made by the individual along with input from a specialist.

REFERENCES
- Hypertrophic cardiomyopathy. American Heart Association. Accessed May 29, 2019
- Prevention and treatment of cardiomyopathy. American Heart Association. Accessed May 29, 2019.
- Maron MS. Hypertrophic cardiomyopathy: Nonpharmacologic treatment of left ventricular outflow tract obstruction. https://www.uptodate.com/contents/search. Accessed May 29, 2019.
